Do Biopsies Spread Cancer?
By Dr. Jonathan Psenka
Quick Summary:
Many people worry that a needle biopsy might cause cancer to spread, and research suggests that while this risk may exist, it appears to be relatively low. Biopsies remain essential because they provide critical information about a tumor, helping doctors diagnose cancer and choose the most effective treatments. Studies in breast and prostate cancer have shown that biopsies can trigger inflammation and other biological changes that may make cancer cells more likely to spread. Research has also found that some patients experience an increase in circulating tumor cells after biopsy, which may be linked to disease progression. Scientists believe that reducing inflammation around the time of biopsy may help lower this risk. Both prescription medications, such as Celebrex, and natural anti-inflammatory compounds, including curcumin, omega-3 fatty acids, and ginger, have shown promise in reducing cancer-related inflammation. Overall, while biopsies may carry some risk of promoting cancer spread, their benefits for diagnosis and treatment planning far outweigh the potential drawbacks, making them an important part of modern cancer care. Keep reading below for the details.
Many people facing a cancer diagnosis question if a needle biopsy may increase the risk that their cancer may spread or metastasize. Sometimes this is referred to as “tumor seeding,” and unfortunately for some people, the biopsy procedure may indeed facilitate the spread of cancer. However, a biopsy can provide very important information, such as tumor type, growth rate, presence of hormone or growth factor receptors, and more that can help determine what the best treatment options are. Biopsies are also used to differentiate between cancerous tissue and benign tissue that may look suspicious on imaging. Therefore, foregoing a biopsy would result in a significant treatment disadvantage.
Current medical literature suggests two ways that cancer may spread during biopsy. One is a process in which the physical disruption to the tumor by insertion of a needle causes a local inflammatory cellular response, causing tissue changes that promote progression of disease. The second is called needle track seeding and in this process cancer cells are physically dragged out of a tumor by the biopsy needle when it is withdrawn out of the tumor.
It is largely unknown how many patients may actually experience a worsening of their cancer due to biopsy. While the likelihood of spreading cancer through a biopsy is thought to be very low, the truth is unknown. This is a hard thing to study as there is no way to tell when a metastatic tumor, which can be started by a single cell, might have first formed, ie. before or after a biopsy. Imaging can’t identify abnormalities at a cellular level; a tumor must be approximately 2-3-mm to be seen, at which point it is comprised of between 100,000 and 1 billion cells. Not all metastatic sites can be blamed on biopsies either, as most cancers have the potential to spread as part of the disease process.
Most people will require only a single needle biopsy to properly diagnose cancer. However, in some types of cancer, such early-stage prostate cancer, where men may adopt a “watch and wait” approach to treatment, multiple needle biopsies are recommended to monitor for tissue changes determining when treatment should begin.
The good news is that science has provided us with information that can help reduce the potential of biopsy-induced cancer metastasis.
In a 2023 study titled “Needle Biopsy Accelerates Pro-Metastatic Changes and Systemic Dissemination in Breast Cancer: Implications for Mortality by Surgery Delay” (Yikes!) data from over 175,000 patients was analyzed for mortality risk based on the time between biopsy and surgery. Their initial findings determined that compared to patients who underwent surgery within 30 days of needle biopsy, the mortality risk rose by 6% at 60 days, 29% at 90 days, and more than doubled by 150 days in those patients who delayed surgery. These findings suggested that delayed surgery may allow biopsy-induced tumor changes to accelerate cancer progression.
The researchers then conducted additional studies using tumor-bearing mouse models of estrogen receptor positive (ER+) breast cancer cells. In the mice that underwent biopsy, there were significantly higher levels of cancer cells spreading to the lungs compared to unbiopsied tumors. The researchers also found that the biopsy did not increase tumor growth directly, but rather that the biopsy triggered biological changes that promoted metastasis rather than simply releasing cancer cells mechanically. After biopsy, tumors developed persistent inflammation and hypoxia (a lack of oxygen) around the wound site. This inflammation and hypoxia attracted immune cells called macrophages, which in turn released signaling molecules that promoted tumor growth and metastasis.
Simply put, the tumor tissue was wounded by the needle biopsy, and this triggered a wound-healing response that allowed the cancer cells to grow and spread.
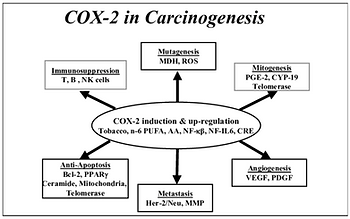
Specifically, the wound of the biopsy caused the injured cells to release inflammatory mediators such as cyclooxygenase 2 (COX-2), prostaglandin E2 (PEG2), and the prostaglandin E2 receptor (EP2). These mediators then caused the macrophages to produce factors such as vascular endothelial growth factor (VEGF) and transforming growth factor beta (TGF-β). This then triggered the formation of new blood vessels in the tumor and promoted epithelial-to-mesenchymal transition (EMT), a process in which cancer cells become more invasive and mobile.
Finally, the researchers examined the effect of performing a biopsy while concurrently using a drug, celecoxib (Celebrex), which specifically inhibits the pro-inflammatory enzyme COX-2. The use of celecoxib was found to significantly reduce metastasis, decrease inflammatory macrophage accumulation, and suppressed EMT around the biopsy wound.
Overall, the study revealed that diagnostic needle biopsy can create a tumor environment that promotes breast cancer progression and metastasis. The findings also show that inhibiting biopsy-associated inflammation can significantly reduce this risk.
Increased risk of prostate cancer progression may also be promoted by biopsy. Prostate cancer is one of the most common cancers affecting men worldwide. Modern medicine has made major advances in diagnosing and treating prostate cancer, yet recurrence rates remain high, with nearly half of patients experiencing persistent disease after treatment.
The standard method for diagnosing prostate cancer is the transrectal ultrasound-guided biopsy (TRUS). As in breast cancer, prostate biopsies are valuable for determining whether cancer is present and also how aggressive the cancer may be. However, studies suggest that the repeated puncturing of tumor tissue may unintentionally dislodge cancer cells into the bloodstream or surrounding tissues.
Roughly 60% of men diagnosed with prostate cancer will choose a “watch and wait” approach or “active surveillance” instead of immediately pursuing cancer treatment. Active surveillance is used in low-to-moderate risk prostate cancer, as determined by an initial biopsy, and involves regularly scheduled monitoring of blood PSA levels, MRI imaging, and repeat prostate biopsies. The idea is that with active surveillance, progression of prostate cancer can be detected early, mainly via biopsy, and treatment can begin before the cancer becomes too advanced.
Researchers have found that prostate biopsies can increase the number of circulating tumor cells (CTCs) in the bloodstream shortly after the procedure. CTCs are cancer cells that have detached from the primary tumor and entered the circulation. Several studies reported that 20–30% of prostate cancer patients experienced elevated CTC levels after biopsy, while another study found increased epithelial cellular material in more than 80% of patients following biopsy.
One major study from 2020 tracked prostate cancer patients for approximately three and a half years after biopsy. Researchers found that patients who experienced increased CTC levels after biopsy were significantly more likely to develop disease progression compared to those without increased CTCs. About 45% of patients with biopsy-induced CTC increases experienced progression, compared to only 15% of patients without increased CTCs. These findings suggest that the mechanical disruption caused by biopsy may adversely influence long-term outcomes in some men with prostate cancer. The study emphasized that patients should not avoid biopsies, since early diagnosis and treatment are still critical for survival. However, researchers suggest that the medical community should more carefully study the possible long-term effects of biopsy-related cancer cell dissemination.
From the research, it is clear that biopsies in both breast and prostate cancer have the potential to stimulate progression and metastasis of cancer. However, at this time the information provided by a tumor biopsy is indispensable in guiding effective treatment selection.
Patients questioning the need for a biopsy often ask the question, “what would you do if you were in my position?” The first thing I would do would be to completely understand the role that biopsies serve in cancer diagnosis and treatment. Second, I would consider ways that could inhibit the inflammation (COX-2, PEG2, VEGF, etc) that is associated with a biopsy. This would include using medications like Celebrex. Like most medications, there is a risk of adverse effects, like heart or gastrointestinal issues, but these are generally seen in people using high doses or taking the medication for a prolonged period.
Additionally, I would consider using some natural COX-2 inhibitors as well. Substances like curcumin, an extract from the spice turmeric, ginger, and omega-3 fats have all been shown to suppress COX-2-related inflammation. Natural COX-2 inhibitors offer a potential advantage over drugs like Celebrex, in that the mechanism they use to inhibit inflammation is different. Meds like Celebrex work by inhibiting a enzyme called cyclooxygenase that converts the omega-6 fatty acid into pro-inflammatory prostaglandins, like PEG2. Some of the natural COX-2 inhibitors also work by inhibiting cyclooxygenase, but others work to inhibit COX-2 at a transcriptional level. Inhibition at a transcriptional level means that the attempt to produce inflammation is turned off at a genetic level, ie. the body doesn’t even make cyclooxygenase in the first place. By using conventional medication along with natural inhibitors, it may be possible to create a more robust anti-inflammatory signal to inhibit cancer progression with biopsy. So, that’s what I would do.

Curcumin, the extract from turmeric, is an amazing natural substance. It has shown the ability to inhibit COX-2 at the transcriptional level, inhibit a molecule known as TNF-beta (another pro-inflammatory molecule frequently elevated in cancer), and inhibit lipoxygenases (LOX). In phase 1 clinical trial, 3.6 grams of oral curcumin were given to people with advanced colorectal cancer. The trial found that there was a 62% decrease in PEG2 within an hour of taking the curcumin. A meta-analysis of 32 clinical trials of over 2000 people confirmed curcumin’s ability to inhibit cancer promoting inflammation.
Omega-3 fatty acids have a significant anti-COX/PEG2 effect. Most commonly taken as fish oil, the omega-3 fats have another name, essential fats. They are essential because the human body requires these fats to operate correctly. However, humans cannot make these fats; they need to be consumed in the diet. Dietary sources of omega-3’s include cold water fish, like salmon, nuts like raw walnuts, and seeds like flax, among others (scroll down on this link for a list). Numerous studies (1, 2, 3) have confirmed the efficacy of omega-3 fats in preventing disease, inhibiting inflammation, and having an anti-cancer effect. One of the omega-3’s, docosahexaenoic acid (DHA) is particularly effective at shutting down COX-2. Salmon contains some of the highest levels of DHA, but a person can only eat so much salmon, so a “high DHA” fish oil supplement is often a good idea.
Ginger too has a well-established anti-COX-2 ability. Interestingly, ginger has possibly the most selective ability to inhibit COX-2, while not inhibiting the beneficial COX-1 enzyme. COX-1 enzymes serve beneficial actions in the body, such as maintaining stomach and kidney health. A meta-analysis of human trials found that 500mg twice daily significantly inhibited inflammation after 2-3 months.
Another advantage the natural anti-inflammatories have is that they have a well-established safety profile and can, and likely should be used for extended periods of time. Indeed, the ability of these natural substances to not only provide an anti-inflammatory effect but also provide the body with essential nutrients makes them excellent candidates for any health-promoting, disease-preventing health plan. Regularly consumption of the dietary sources of these compounds should be a goal for anybody wanting to be health.
So, do biopsies spread cancer? The answer is, unfortunately, yes. However, biopsies do provide crucial information regarding tumor characteristics that can be used to create successful treatment plans. To minimize the risk of biopsy promoting cancer progression, it would be a good idea to create a strong anti-inflammatory state within the body before the procedure. Further, adopting a conservative approach to biopsy frequency in favor of other monitoring tests should be considered. Imaging such as MRI, and blood tests evaluating circulating tumor cell levels are showing promise as non-invasive cancer monitoring modalities. The long-term safety of the natural anti-inflammatories, along with their anti-cancer action, suggests that continuing their use after biopsy and during treatment, and in the prevention of recurrence stage of fighting cancer is a smart move.